
How Medicare coverage works for 2026
Medicare doesn't hand out assistive tech just because you've turned 65. To get coverage, your doctor has to prove medical necessity, certifying that a specific device is the only way to manage your health. It's a bureaucratic process that requires more than a simple request.
Medicare is divided into four parts: A, B, C, and D. Parts A and B, often called Original Medicare, cover most durable medical equipment (DME). Part C (Medicare Advantage) plans often include benefits beyond Original Medicare, and Part D covers prescription drugs, which can sometimes be relevant for devices like medication dispensers. It’s crucial to understand your specific plan’s coverage.
The situation for 2026 appears to be a continuation of recent trends – expansion of coverage in specific areas, like hearing aids, coupled with increased scrutiny of DME claims. The Centers for Medicare & Medicaid Services (CMS) is constantly updating guidelines, and we’re seeing a greater emphasis on value-based care and preventing hospital readmissions. This means devices that demonstrably improve health outcomes and reduce healthcare costs are more likely to be covered.
CMS guidelines from late 2024 set the baseline for what we expect in 2026. Because regional policies vary, you should verify these details with your specific plan provider before making a purchase.
Wheelchairs, walkers, and mobility limits
Wheelchairs, scooters, walkers, and canes are among the most frequently covered assistive devices by Medicare. However, getting approval requires a doctor’s prescription detailing a significant limitation in your ability to move around – meaning you have difficulty with activities of daily living even with the aid of a device. A simple preference for a wheelchair isn’t enough.
There’s a big difference between standard and power wheelchairs, and that impacts coverage. Standard wheelchairs are generally covered more readily if you can self-propel or have someone available to assist. Power wheelchairs require more justification, typically demonstrating a severe mobility impairment where self-propulsion isn’t possible. You’ll need a detailed evaluation from a physician or physical therapist.
It’s important to know what Medicare doesn’t cover. Stairlifts, for example, are considered home modifications and aren’t typically covered by Original Medicare. Similarly, modifications to your home to accommodate a wheelchair, like widening doorways, aren't covered. These are generally considered your responsibility.
Medicare utilizes a Competitive Bidding Program for certain DME, including wheelchairs and walkers. This program aims to lower costs by having suppliers compete for contracts. This can affect your choice of providers and the price you pay, even after Medicare’s portion is covered. You can find a list of contracted suppliers on the Medicare website.
- Standard wheelchairs are covered with a basic prescription.
- Power wheelchairs require documentation showing you cannot use a manual chair.
- Walker/Cane: Covered if they improve mobility and safety.
- Scooter: Coverage similar to power wheelchairs, requiring significant mobility limitations.
Medicare Coverage for Common Mobility Aids - 2026
| Device Type | Typical Medicare Coverage | Required Documentation | Approximate Cost (without Medicare) |
|---|---|---|---|
| Manual Wheelchair | Medicare Part B generally covers manual wheelchairs if a doctor prescribes one because of a medical necessity. Coverage requires a physician’s prescription and documentation demonstrating the need. | Prescription, Certificate of Medical Necessity (CMN) completed by the prescribing physician, documentation from supplier. | $800 - $2,000+ |
| Power Wheelchair | Medicare Part B covers power wheelchairs for individuals with significant mobility limitations who meet specific criteria. A thorough evaluation is required to demonstrate medical necessity. | Prescription, Detailed Medical Justification, CMN, supplier documentation, and potentially a Physical or Occupational Therapy evaluation. | $2,000 - $6,000+ |
| Scooter (Portable Oxygen) | Medicare Part B may cover scooters for those who have difficulty walking but can safely operate a scooter. Medical necessity must be established. | Prescription, CMN, documentation of medical condition limiting mobility, supplier documentation. | $800 - $3,000+ |
| Walker | Medicare Part B covers walkers if a doctor prescribes one as medically necessary to assist with ambulation. | Prescription, CMN, documentation supporting medical need. | $100 - $300+ |
| Cane | Medicare Part B covers canes when prescribed by a physician as a medically necessary assistive device for ambulation. | Prescription, CMN, documentation supporting medical need. | $20 - $100+ |
Illustrative comparison based on the article research brief. Verify current pricing, limits, and product details in the official docs before relying on it.
New rules for hearing and vision
Medicare coverage for vision and hearing aids has been expanding, albeit slowly. For vision, Medicare Part B covers an annual dilated eye exam for people with diabetes. It also covers eyeglasses or contact lenses following cataract surgery. However, routine vision care, like exams for prescription updates, isn’t covered.
The biggest change is with hearing aids. While Medicare traditionally didn't cover hearing aids, the 2026 guidelines are expected to include coverage for hearing evaluations and fitting services performed by audiologists. The actual cost of the hearing aids themselves may be partially covered, with cost-sharing requirements.
However, there are limitations. Coverage for hearing aids typically requires a hearing exam and a fitting by a licensed audiologist. The hearing aid must also meet certain criteria, and you’ll likely have a deductible and co-insurance to pay. It’s not a free benefit, but it makes hearing aids significantly more accessible.
Low vision aids like screen readers are covered when they are necessary for daily tasks. Smart glasses remain in a gray area; Medicare hasn't established clear reimbursement codes for them yet, so coverage is unlikely in most regions for 2026.
It's important to note that the expansion of hearing aid coverage is relatively new, and the details are still being worked out. The CMS website provides the most up-to-date information on what’s covered and what isn’t.
Fall prevention and home safety
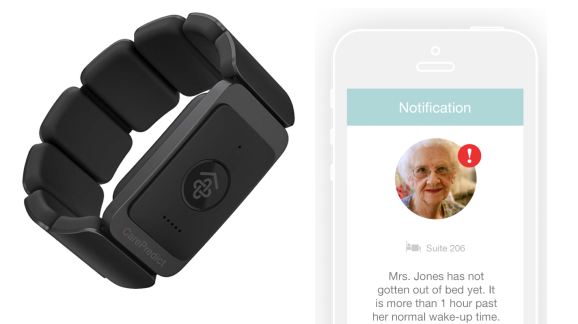
Falls are a major concern for seniors, and Medicare covers several devices and services aimed at preventing them. Fall detection systems, which automatically alert emergency services if a fall is detected, are becoming increasingly popular. Medical alert buttons, which allow you to manually call for help, are also covered.
Medicare Part A covers some home healthcare services, such as physical therapy and occupational therapy, which can help seniors improve their balance and strength. A home safety assessment, performed by an occupational therapist, can identify potential hazards and recommend modifications to reduce the risk of falls.
However, Medicare generally doesn’t cover structural home modifications like installing grab bars in the bathroom or building ramps. These are considered home improvements and are typically the responsibility of the homeowner. Some Medicare Advantage plans may offer limited coverage for home modifications, so it’s worth checking your plan details.
Investing in a well-lit home, removing tripping hazards like loose rugs, and ensuring clear pathways can also significantly reduce the risk of falls. These simple steps, combined with assistive devices and home healthcare services, can help seniors stay safe and independent in their own homes.
Communication & Cognitive Aids
For seniors with communication or cognitive impairments, Medicare covers a range of assistive devices. Amplified telephones, which increase the volume of incoming calls, are a common example. Teletypewriters (TTYs) are also covered for individuals with hearing or speech impairments, allowing them to communicate over the phone using text.
Devices for people with dementia or Alzheimer's disease are covered on a case-by-case basis, depending on medical necessity. This might include memory aids, communication boards, or devices that provide reminders and prompts. Coverage often requires documentation from a physician or neuropsychologist.
A speech-language pathologist plays a crucial role in recommending and fitting communication aids. They can assess your needs and help you choose the device that’s best suited for your specific condition. Medicare covers speech-language pathology services when they’re deemed medically necessary.
Brain training apps and cognitive software rarely meet the definition of durable medical equipment. While some Medicare Advantage plans include them in wellness packages, Original Medicare does not currently pay for these digital tools.
Covered Assistive Devices
- Durable Medical Equipment (DME) - Medicare Part B generally covers 80% of the cost of DME, if your doctor prescribes it and the supplier is enrolled in Medicare. This includes items like walkers, wheelchairs, hospital beds, and commodes.
- Oxygen Equipment & Supplies - If a doctor prescribes oxygen due to a respiratory condition, Medicare Part B covers up to 80% of the cost of oxygen equipment and supplies, including oxygen tanks, concentrators, and tubing.
- Blood Glucose Monitors & Testing Supplies - For beneficiaries with diabetes, Medicare Part B covers the cost of blood glucose monitors, test strips, and lancets if certain conditions are met, often requiring a prescription and enrollment in a Medicare-approved diabetes self-management training program.
- Mobility Scooters - Medicare Part B may cover the cost of a mobility scooter if it is deemed medically necessary by a physician. Coverage requires a prescription and often a prior authorization.
- Hearing Aids (Limited Coverage) - While traditional Medicare doesn’t cover routine hearing exams or hearing aids, some Medicare Advantage plans *do* offer benefits for hearing care, including hearing aid coverage. Check with your specific plan.
- Communication Devices - For individuals with speech or language impairments, Medicare may cover augmentative and alternative communication (AAC) devices, but these typically require extensive documentation and prior authorization.
- Canes - A cane is considered DME and is generally covered by Medicare Part B at 80% of the Medicare-approved amount when prescribed by a doctor.
Durable Medical Equipment: Beyond the Basics
Beyond wheelchairs and walkers, 'Durable Medical Equipment' (DME) encompasses a wide range of devices. Hospital beds are covered when a physician determines that you require a bed that can be adjusted for various positions to manage your medical condition. Oxygen equipment is covered for individuals with chronic respiratory illnesses, but requires a prescription and ongoing monitoring.
Patient lifts are covered when you have limited mobility and require assistance getting in and out of bed or a chair. Coverage typically requires documentation from a physician or physical therapist. The DME must be prescribed by a doctor and obtained from a Medicare-approved supplier.
Getting DME covered involves a specific process. Your doctor must write a prescription, and the supplier must be enrolled in Medicare. Medicare will then review the claim to determine if the equipment is medically necessary and meets their coverage criteria. Be prepared to provide documentation to support your claim.
Medicare conducts DME audits to ensure that suppliers are complying with regulations and that equipment is being provided appropriately. If your claim is denied, you have the right to appeal. Understanding the difference between "rental’ and ‘purchase" options for DME is also important. Some equipment is covered for rental only, while others can be purchased.
Which type of Medicare-covered assistive technology do you find most helpful or would like to see covered more comprehensively?
As Medicare expands its coverage of assistive technologies in 2026, we want to hear from you. Which category of devices matters most to your daily life and well-being? Your feedback helps us focus on the topics that matter most to our senior community. Vote below!
Navigating the Appeals Process
If your claim for assistive technology is denied by Medicare, don’t give up. You have the right to appeal the decision. The appeals process has several levels, starting with a redetermination by your Medicare contractor. If that’s unsuccessful, you can request a reconsideration by an independent review entity.
The next level is an administrative law judge hearing. If you’re still unsatisfied, you can appeal to the Medicare Appeals Council. As a final step, you can file a lawsuit in federal district court. Each level has specific deadlines, so it’s crucial to file your appeal promptly. Missing a deadline can result in your appeal being dismissed.
Preparing a strong appeal requires gathering supporting documentation, such as your doctor’s prescription, medical records, and any other evidence that demonstrates the medical necessity of the device. Write a clear and concise letter explaining why you believe the denial was incorrect. Focus on how the device will improve your health and quality of life.
State Health Insurance Assistance Programs (SHIPs) offer free counseling and assistance with Medicare appeals. They can help you understand your rights, gather documentation, and navigate the appeals process. You can find your local SHIP by visiting the Medicare website or calling 1-800-MEDICARE.


No comments yet. Be the first to share your thoughts!